MISLEADING CLAIMS
Issues | Did RFK Jr cause a measles outbreak in Samoa?
Synopsis
Several stories report that RFK Jr is responsible for a 2019 measles outbreak in Samoa that resulted in over 5,000 cases and 83 deaths. It is widely believed that the outbreak stemmed from low vaccination rates preceding it. Numerous articles have surfaced recently (c. November 2024) alleging that RFK Jr and his advocacy group, Children’s Health Defense (CHD), are to blame for the lack of vaccine coverage in Samoa. These claims primarily focus on three assertions:
- CHD exploited the deaths of two infants to raise questions about vaccine safety, creating mistrust and reducing vaccine uptake.
- RFK Jr’s June 2019 visit to Samoa discouraged vaccination, further contributing to vaccine hesitancy.
- In a November 2019 letter to the Samoan Prime Minister, RFK Jr deflected blame from the anti-vaccine movement by suggesting the outbreak was caused by a defective vaccine.
This investigation evaluates these claims by examining the timeline of events, vaccination rates, and systemic factors contributing to the outbreak.
Background
Several stories report that RFK Jr bears responsibility for a 2019 measles outbreak in the island nation of Samoa that resulted in more than 5,000 cases and 83 deaths. For example, on PBS NewsHour, Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia and member of the FDA advisory committee on vaccines, asserts RFK Jr “had everything to do” with the outbreak:
Now, very quickly, within two weeks, it was realized what that mistake was [that caused two infant deaths in Samoa within minutes of receiving MMR vaccines in 2018]. It was a nursing error. But, nonetheless, RFK Jr seized on that. He flooded Facebook with information that measles vaccine is killing children in Samoa. He went to Samoa. He met with anti-vaccine activists. He met with senior officials in Samoa and kept the drumbeat alive that measles vaccine was killing children in Samoa.
As a consequence, vaccination rates fell from 70 percent to 30 percent. And between September and December of 2019, there was a massive measles epidemic. In this island nation of 200,000 people, there were 57,000 cases of measles and 83 deaths. Most of those deaths were in children less than four years of age.
And Robert F. Kennedy Jr had everything to do with that. And that shows you how disinformation can kill.
Before considering whether RFK Jr was responsible for the 2019 Samoa measles outbreak and the deaths of 83 people, a brief overview is necessary.
2018 infant deaths in Samoa following MMR vaccines
On July 6, 2018, two babies brought to a hospital in Samoa died within minutes of receiving MMR (measles-mumps-rubella) vaccines.
The government suspended the MMR program days later and called for a full investigation. However, the inquiry was put on hold until the trial of the two nurses who administered the vaccines was completed.
It wasn’t until April of 2019 when the Director of Health announced that human error caused the death of the two infants. The MMR program was restarted later that month — more than nine months after the suspension began — but only at hospital clinics.
In July, the Director of Health said that every vial of the vaccine should be mixed with one vial of diluent, but the vaccine was mixed with something else.
In August, the two nurses were sentenced to five years in prison, and it was confirmed that one of the nurses mistakenly mixed the MMR vaccine powder with an expired skeletal muscle relaxant (atracurium).
The MMR vaccine used in Samoa is delivered in vials containing five doses in the form of a freeze-dried powder and is supplied with a diluent (sterile water). The vaccine needs to be reconstituted prior to administration.
Nurses Luse Emo Tauvale and Leutogi Te’o, were sentenced to five years in prison for negligence causing manslaughter over the death of two one-year-olds: a girl and a boy.
Luse is the individual who mixed the powder of vaccine with atracurium. According to reports, the vaccination of the girl was performed by a trainee nurse under Luse’s supervision.
Soon after leaving the clinic with her daughter, the mother noticed rapid changes to her baby while waiting for a bus home.
“Her baby’s body felt cold; her eyes could not open properly and her legs were [spasming] out; she rushed back to the Hospital for assistance and the nurses, including the defendants, tried to revive the baby but the young baby stood no chance,” Justice Vui said.
“She passed away.”
Justice Vui said, at this point, applicable nursing protocols required that further vaccinations at the Hospital should have stopped following the death of a previously healthy baby.
“It appears from the material the defendants did not recognise the possibility the problem was the vaccine,” he said.
The defendants told the Probation Office they concluded the baby was allergic to the vaccine.
“They concluded without any evidence to support their theory; a conclusion plucked out of thin air,” the Acting Chief Justice said.
The second defendant, Leutogi, concluded that the child must have been suffering from a prior illness.
Justice Vui characterised this as a “clearly callous observation unsupported by evidence”.
For the second nurse, Leutogi, “the Acting Chief Justice said her crime related to negligence in her duties as a Nurse Manager and her role in persuading the mother of the second baby, the boy, to have the vaccine after she objected to having her child vaccinated,” according to the Samoa Observer. “And so Luse told her if that was case, she would need to sign a refusal to consent form; at this point Leutogi then convinced the mother to have her child vaccinated,” the Chief Justice said.
Police said Leutogi was warned by the other nurses not to but used the same mixture that had been administered to the first child earlier that morning and the nurse proceeded to personally administer the vaccine to the baby.
Like the first case earlier that morning, the boy’s conditioned rapidly deteriorated.
“Efforts to save this young baby stood no chance,” the Chief Justice said. “It took the death of the second child before the defendants to finally realise the problem laid not on the children but the supposedly safe vaccine.”
Luse retraced her steps to the rubbish bin and retrieved the anaesthetic and syringes, where she noticed that the wrong bottle had been used to mix the vaccine and that it was expired.
“Fear for consequences for her [led her to conceal] the vial and rest of the vaccine in a plastic bag and put it in her pocket; [she] said nothing to anyone about what she had discovered,” Justice Vui said.
“And she took the materials home. She kept this information until two weeks later when she disclosed the police investigators what had occurred.
About a month after the tragedy, the Director General said in response to the first court hearings for one of the nurses (Luse) charged with manslaughter, “Well, from what I gather it is human error,” Newshub reported. “With this type of tragedy, we wouldn’t want to rush.” However, it wasn’t until the MMR vaccination program resumed in April of 2019 — about 10 months after the deaths — that the Samoan Director General of Health confirmed that it was a nursing error.
2019 Samoa measles outbreak
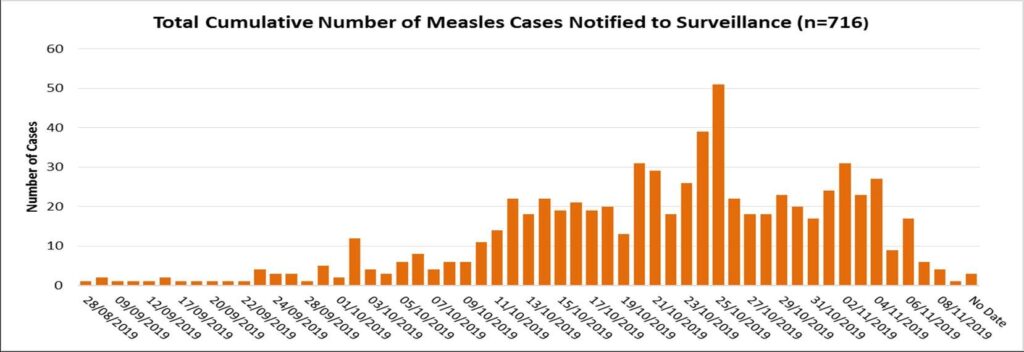
On October 16, a measles outbreak was declared as four specimens from September 30 were positive. Government data later released publicly showed that Samoa had one case of measles reported to surveillance on August 28, as depicted in Figure 1 below.
On November 15, a State of Emergency was declared. Some criticized the government for reportedly waiting six weeks and more than 200 cases before declaring an SoE and reporting these cases publicly.
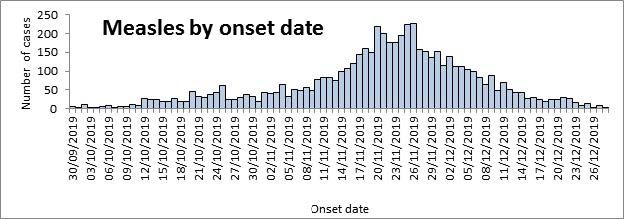
A mandatory mass vaccination campaign followed, including a two-day nationwide lockdown in December, during which vaccination teams went door-to-door. The State of Emergency ended at the end of the year. As of January 2020, there were about 5,700 reported cases and 83 measles-related deaths, mostly in children. Figure 2 below shows measles cases roughly between September and late December.
Cause of the outbreak
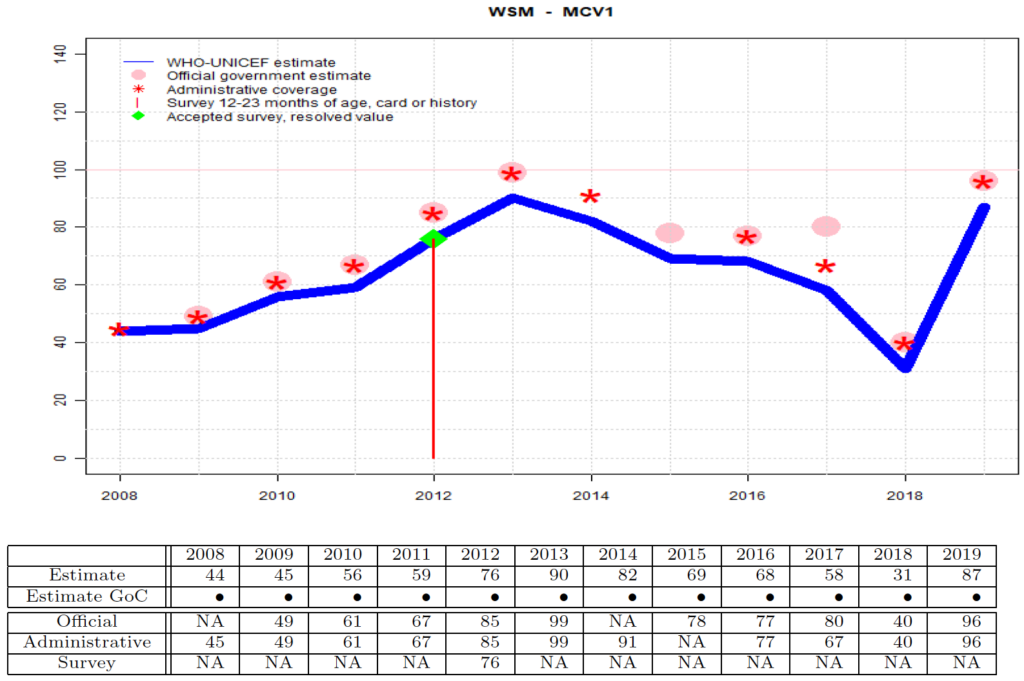
The cause of the outbreak was attributed to decreased vaccination rates, falling from 58% in 2017 to 31% in 2018, according to WHO and UNICEF estimates, as shown in Figure 3 below.
What precipitated such a sharp decline? This was “largely due to misinformation and mistrust among parents,” according to UNICEF and the WHO’s Director of the Department of Immunization, Vaccines and Biologicals, Katie O’Brien.
Officials blamed the low rates in part on fears sparked after the two infants died after receiving MMR vaccines. This diminished parents’ trust in the safety of the vaccine, even though it turned out that the deaths of the two infants were caused by human error.
“O’Brien said that an anti-vaccine group had been stoking these fears further with a social media campaign, lamenting that ‘this is now being measured in the lives of children who have died in the course of this outbreak,’” according to The Guardian. “Misinformation about the safety of vaccines, she said, ‘has had a very remarkable impact on the immunisation programme’ in Samoa.”
Claims implicating RFK Jr in the 2019 Samoa measles epidemic
Numerous articles have surfaced recently (c. November 2024) holding RFK Jr and Children’s Health Defense (CHD), the advocacy group that Kennedy founded, responsible for the lack of vaccine coverage in Samoa. The arguments these authors — and institutional organizations — make can be boiled down to three central claims:
- RFK Jr (and CHD) exploited the deaths of two infants to raise questions about vaccine safety on social media, causing mistrust and a decline in vaccine coverage
- During his visit to Samoa in the summer of 2019, RFK Jr directly or indirectly discouraged people from getting vaccinated, causing a decline in vaccine coverage. He promulgated misinformation or lent credibility to local anti-vaxxers, or both, leading to increasing vaccine hesitancy among Samoans.
- In his letter to the Samoan Prime Minister, RFK Jr deflected blame from the anti-vaccine movement and instead spread misinformation by suggesting the outbreak was caused by a defective vaccine.
Claim 1 | RFK Jr (and CHD) exploited the deaths of two infants to raise questions about vaccine safety on social media, causing mistrust and a decline in vaccine coverage
Claim 1 | Synopsis
The claim centers on CHD’s alleged Facebook posts questioning vaccine safety after two infant deaths in July 2018. Following these deaths, Samoa’s government suspended the MMR vaccination program for 10 months, resuming only in April 2019. Annual vaccination coverage for 2018 was 31% due to this suspension. Critics argue that CHD’s social media activity and alleged fearmongering caused mistrust among parents, further contributing to the decline in vaccine uptake. However, the timeline indicates vaccination rates dropped due to program unavailability rather than parental mistrust.
Parental mistrust after the infant deaths, especially over the weekend when news began to spread, was warranted. The deaths of two infants from the same vial of the MMR vaccine understandably raised alarms among parents, exacerbated by images shared on social media, such as photos of a grieving mother holding her deceased child. Although the subsequent investigation revealed that the deaths were caused by improper vaccine administration — where a muscle relaxant was mistakenly used as a diluent instead of sterile water — this clarification did little to assuage fears. Parents justifiably questioned how such a grave error could occur and whether they could trust the healthcare system to administer vaccines safely in the future.
Claim 1 | Introduction
An article in the Washington Post published on November 27, 2019, asserts that CHD questioned the safety of the infants’ vaccines on social media. “In several Facebook posts in July and August 2018, Children’s Health Defense, the advocacy group that Kennedy founded, questioned the safety of the vaccines the infants received,” according to the WaPo. “The charity did not update the posts to explain the nurses’ error to its audience.”
Paul Offit, quoted at the top of this article, said RFK Jr “flooded Facebook with information that measles vaccine is killing children in Samoa.” (We’ll assume he means CHD because RFK Jr made no posts related to MMR vaccine use in Samoa in 2018 or 2019 nor are there any posts related to the measles outbreak in 2019 on his personal page. However, this also assumes that no such posts were once present and subsequently deleted.)
“Children’s Health Defense, the nonprofit anti-vax outfit he led until becoming a presidential candidate,” writes David Corn in Mother Jones, “had helped spread misinformation that contributed to the decline in measles vaccination that preceded the lethal eruption.”
A WHO official said that an anti-vaccine group had been stoking the fears of Samoan parents with a social media campaign. While the official doesn’t identify the group, we’ll assume it is a reference to CHD for the sake of the argument. Several more articles make the same claim.
In 2022, Facebook removed the CHD account, and their posts are no longer available. If the page were still active, we would find all relevant posts and share links here (assuming none had been deleted or removed). Without these posts, it’s challenging to address the following essential questions:
- Did the CHD Facebook page publish posts addressing the infant deaths in Samoa? (If so, what did they say?)
- Assuming they did, what are the dates of the posts?
Did the CHD Facebook page publish posts addressing the infant deaths in Samoa? (If so, what did they say?)
Can we take it as a given that CHD questioned on their Facebook page the safety of the vaccines the infants received? Yes. The “vaccines” link provided by the WaPo at the beginning of this section (“In several Facebook posts in July and August 2018, Children’s Health Defense, the advocacy group that Kennedy founded, questioned the safety of the vaccines the infants received”) is broken. However, the URL was retrievable via Wayback Machine [perma]. WaPo links to an August 5, 2019, link post by CHD that says:
Vaccine safety science needed. Were these once-healthy children who died the only two to receive MMR that day? If not, why were they the ones to die? Research needs to determine susceptibility so that no child is ever injured. “The case shakes faith in Samoan health system. The emotionally charged case sparked fears in Pacific nation about the safety of vaccinations, with the Samoan Government issuing an immediate recall on the MMR vaccine.”
A link post includes a URL, generating a link preview with an image, headline, and description. CHD links to an August 2, 2019, article by the Australian Broadcasting Corporation entitled, “Samoan nurses jailed over deaths of two babies who were given incorrectly mixed vaccines.” The quoted text from CHD’s post is from this story. The image from the link preview isn’t visible on the archived page, only a gray rectangle where the image is customarily displayed (you can still click in this area and visit the article), but a title and description are present if you look toward the bottom of the page. Facebook has a Sharing Debugger page that allows you to enter a URL and generate a Link Preview to see the link preview created when your Facebook post is published. So we can use this to show the image:

The Debugger also provides the same description as shown on the archived page: “The nurses pleaded guilty to manslaughter after they injected two babies with incorrectly mixed vaccinations in July last year.” What’s odd is that the WaPo uses a post by CHD from August 2019 when referring to Facebook posts they claim were made in August and July of 2018. Not only that, the WaPo also asserts, “The charity did not update the posts to explain the nurses’ error to its audience.” However, the WaPo cites a CHD post that links to an article reporting the nurses’ error and their sentencing. Anyone viewing the post can read the full story provided by CHD or even read the subheading displayed on the post. So unless the WaPo means that CHD didn’t make retroactive changes and edit the content of their older posts, their claim is contradicted by the evidence they provide.
What are the dates of the Facebook posts?
We don’t know whether or when CHD made posts related to the infant deaths before the one dated August 5, 2019, that the WaPo provided. The WaPo claims CHD made several posts in July and August of 2018. However, the critical time window is much shorter: between July 6 and July 9, 2018.
Here’s why. On Friday, July 6, the two infants died, and then on Monday — three days later — when the deaths were first reported. This was the same time that the Samoan Prime Minister called for a full investigation into the deaths, and the Samoan Director General of Health recalled the MMR vaccine and suspended the vaccine program until the investigation’s completion.
Facebook post from the Government of Samoa — Monday, July 9, 2018, at 6:43 PM (Samoa time):
STATEMENT FROM THE PRIME MINISTER
The following is a statement issued by Prime Minister Tuilaepa Lupesoliai Dr. Sailele Malielegaoi today in response to reports that two young babies died over the weekend in Savaii after being administered with immunization vaccination.
I have not been fully briefed concerning the circumstances leading up to the death of the two innocent young children who passed away reportedly after the young boy and girl were administered vaccination injections at a District Hospital in Savai’i last Friday. But it will not detain me from reiterating a message of sympathy and condolences to the parents and families.
Death leaves a heartache no one can heal. And I can imagine that there is no pain more far reaching and deeper than losing a child. My heart and prayers go out to the grieving families at this most difficult time. To that effect, I humbly extend my deepest sympathy, condolences and pray that comfort and peace will come to them
As a grandfather and father, I can relate to the grief by the families for their loss.
I also almost lost one of my grandsons several years ago under similar circumstances.
But with the Grace of our Father in Heaven, my grandson survived with the proper treatment. But he will never be the same as he has lost the ability to speak.
As Prime Minister, I have called a full inquiry into the circumstances leading up to this devastating incident which I do not take lightly.
There are already processes that will determine if negligence is a factor. And if so, rest assured those processes will be implemented to the letter to ensure that such a tragedy will not be repeated and those responsible will be made to answer.
The deaths also reaffirm the desires behind the government to proceed with the merger between the National Health Services and the Ministry of Health at full speed. When completed, the merge will ensure that incidents of this nature will not be repeated. It is a message to our people that deaths of the two young infants are not in vain.
Providing quality health care for our people remains a key government priority.
To that end, we have just inked a partnership with medical specialists from India ranked as the best medical practitioners in the world to start the second phase of our engagement which will see specialists from India performing state of the art surgeries in Samoa. Six other medical specialists from the People’s Republic of China will soon join our medical staff to share their wealth of experience.
When it comes to the Health Sector, government does not and will not put a price tag on saving our peoples lives. This is reflected by government’s resolve to provide the best and latest lifesaving treatment available for our people. For the government it is not just an obligation but a given.
Again, I extend my sincere condolences to the grieving parents and relatives.
It wasn’t until April 2019 when the Director of Health announced that human error caused the death of the two infants, and the program restarted later that month.
Recall that UNICEF and the WHO (including the WHO’s Director of Immunization) say the decline in vaccination coverage from 2017 to 2018 was “largely due to misinformation and mistrust among parents” related to the July 6 incident.
But how can CHD be laid to blame for a decline in vaccine coverage in Samoa in 2018, given that the first reports of the infant deaths and suspension of the MMR program co-occurred and the measles vaccination program didn’t resume until April 2019?
Also, world health officials blamed the low 2018 rates partly on fears sparked after the two infants. According to them, this diminished parents’ trust in the safety of the vaccine, even though it turned out that the deaths of the two infants were caused by human error.
Again, the timeline cannot support this reasoning.
One, the level of distrust among parents about the MMR vaccine cannot be a factor in the 2018 decline in MMR vaccination rates because the decision whether to vaccinate their children was taken out of their hands — the program was halted almost immediately after the infant deaths and the suspension continued through the end of the year.
Two, the parents were not informed that the deaths of the two infants were caused by human error until the summer of 2019. This timeline makes it unlikely that the revelation influenced parental trust in the MMR vaccine in 2018, as it occurred well after the decline in vaccine coverage that year. Even if some parents had learned about the incident through CHD’s Facebook posts before the government suspended the MMR vaccine program, the extent to which this influenced parental mistrust is uncertain. The program’s suspension, which lasted for the year’s second half, directly reduced access to vaccinations and significantly contributed to the halving of vaccine coverage in 2018.
To be clear, the various articles asserting that CHD’s questioning of the vaccines on Facebook caused a decline in vaccine coverage, all citing a low level of 31% before the measles outbreak in 2019. This was the estimated vaccine coverage in 2018, as shown in Figure 3 above. UNICEF and the WHO are making this same claim.
Since the government acted so swiftly following the infant deaths, CHD and Samoan parents had little more than a day could not have impacted vaccination coverage in 2018, nor could have parents’ mistrust in the MMR vaccine.
While this may seem a reasonable assumption, we haven’t heard from the Samoan government itself. In their 2019 annual report (fiscal year July 2018 to June 2019), the Samoan Ministry of Health says the cause of the government suspension was “fear towards vaccinations on the social media” (p. 42):
On 6 July 2018 in Safotu Savai’i, two 12-month-old children died within hours after receiving MMR vaccinations. This was followed by a period of uncertainty for the EPI [Expanded Programme for Immunization] program as a result of the two recorded cases of Adverse Effects Following Immunisation (AEFI). These two deaths generated fear towards vaccinations on the social media, and other media forms causing the government to suspend its measles vaccination programme. The government recalled and stopped the MMR vaccination programme for 10 months, until it was declared safe to resume when the adverse effects were clarified. The incident may have generated a sense of mistrust in the healthcare system.
These fears about vaccination on social media must’ve been generated over the weekend if the Ministry of Health claims this is the cause of the program’s suspension. Is there any evidence of this on Facebook? None that we could find. However, Facebook may have since removed such material from the site. One observation that gave me pause is that a July 11, 2018, statement by the Samoan government remarked that their Primer Minister’s statement posted to Facebook two days prior had already attracted over 600 comments. We revisited the PM’s statement and found that it had 260 comments (as of December 17, 2024). It’s possible that Facebook removed the most ‘fear-generating’ comments — removing content that goes against their standards.
Nevertheless, we found a July 10, 2018, article from the New Zealand Herald suggesting interaction on Facebook after the infant deaths but before the public announcement of the vaccine program’s suspension:
News of the deaths began to spread over the weekend after family members posted photos of the dead children – one wrapped in the arms of his distraught mother – on Facebook. The public was officially informed by authorities yesterday, when Samoa’s Ministry of Health chief, Dr Leausa Toleafoa Take Naseri, announced that all MMR vaccines in the country were to be seized after the deaths.
The story also explained that the families of the two children had spoken with TV1 Samoa, the country’s leading television station. TV1 Samoa posted a July 8, 2018, update at 9:17 pm EDT (Monday, July 9 at 2:17 pm in Samoa) on Facebook explaining that their news team was en route to visit the hospital where the children received their vaccinations and to meet the families.
Facebook post from — TV1 SAMOA — Monday, July 9, at 2:17 pm (Samoa time):
TALA FOU NEWS UPDATES: Tala Fou News team is on the ground in Savaii heading to Safotu and Sasina to meet the families of the young children who have allegedly died not long after receiving their vaccinations. Our first stop to get latest update from Safotu Hospital where its believed the children received their vaccinations. The staff member informing our reporter that the hospital is not willing to release any information in relation to the deaths of two young children who have allegedly died after receiving their vaccinations. Further stating that the Police investigation into the deaths of the two children is underway and no further information will be released until they can determine exactly what happened. After numerous calls and emails to the Minister of Health and the offices of CEO of the National Health Services and Ministry of Health Tala Fou has just been informed that there will be a press conference at 3pm this afternoon.
This post was the earliest one we could find related to the infant deaths in Samoa. Notice that this same post indicates that TV1 Samoa’s news team (”Tala Fou” is the name of TV1 Samoa’s news program) had been in contact with the Samoan government — and the Director of Health had informed them of a press conference that was to occur within less than hour from the time of their post. Based on the wording of their post, it looks like they may have previously reported or discussed the story on Facebook, but this is the first piece of content from TV1 Samoa on Facebook. The earliest video clip from TV Samoa shared on its Facebook page was posted after the Director of Health’s press conference.
Facebook post from TV1 SAMOA: Monday, July 9, 2018, at 9:59 pm (Samoa time):
BREAKING NEWS – O lea ua faamaonia nei le toe aoina o le vailaau o le MMR lea o loo faia ai tui puipui o fanau iti ua atoa le tausaga le matutua. Faamaonia mai e le Faaton Sili o le Matagaluega o Soifua Maloloina o lea vailaau lea na faaoga e fomai e faia ai tuiga o fanau iti e toalua lea ua maliliu nei. O lea foi ua faamaonia mai ua suesue e Leoleo lea tulaga ona o lea ua faaulu tagi a aiga o ia fanau iti ona o lenei mataupu.
[ChatGPT English translation: It has now been confirmed that the MMR vaccine, used for immunizing young children who have reached one year of age, has been recalled. The Director-General of the Ministry of Health confirmed that this vaccine was used by doctors to administer injections to two young children who have since passed away. It has also been confirmed that the Police are investigating this matter, as the families of these children have filed complaints regarding this incident.]
We still can’t confirm whether CHD posted anything during this time on their Facebook and there’s no evidence that RFK Jr did so on his personal page. We do know the infant deaths were reported before the public release of this information, but that was within minutes of the Director of Health’s press conference, where he announced the recall of the MMR vaccines. Nevertheless, the startling report from the NZ Herald — that news of the deaths spread over the weekend after family members posted photos of the dead children on Facebook — this is not the type of information that a reporter would publish unless there were no uncertainty in the veracity of the incident.
Claim 1 | Conclusions
The alleged role of CHD in reducing vaccine coverage is unsupported by verified evidence. The decline in coverage was caused by the suspension of Samoa’s vaccination program, not external influences. Any purported impact of social media activity during this period is mistaken, as the suspension effectively removed the choice of vaccination from parents.
Parental mistrust of the healthcare system and the MMR vaccine after the deaths was understandable — especially given the tragedy of two infants dying from the same vaccine vial — the root of this mistrust lies in systemic healthcare failures, not external misinformation.
Claim 2 | RFK Jr’s visit to Samoa increased vaccine hesitancy, causing poor vaccine coverage
Claim 2 | Synopsis
This claim alleges that RFK Jr’s June 2019 visit to Samoa, where he met with local vaccine opponents, increased vaccine hesitancy and further reduced vaccination rates. A closer examination reveals that vaccination rates were already very low due to a 10-month suspension of the MMR program — almost assuredly lower than the 31% estimate for 2018 since the suspension continued into the first four months of 2019. Evidence linking RFK Jr’s visit to declining vaccination coverage is weak, and systemic factors, including government delays and mistrust, better explain the low vaccine uptake before the 2019 measles outbreak.
Claim 2 | Introduction
Several articles point to RFK Jr’s June 2019 trip to the country as another reason he is responsible for the lack of vaccine coverage. “Kennedy had publicly supported leading vaccination opponents there,” writes Corn in Mother Jones, “lending credibility to anti-vaxxers who were succeeding in increasing vaccine hesitation among Samoans.”
“Kennedy’s brand of extreme anti-vaccine activism can have deadly consequences,” writes Edward Nirenberg and Gavin Yamey in TIME.
In June 2019, he visited Samoa, appearing alongside local anti-vaccine activists. Later that year, a measles outbreak resulted in 83 preventable deaths, most of which were in children under 5, because of poor uptake of the MMR vaccine.
Most of the stories provide no context. Reading them, it is not unreasonable to assume that Samoa was a stop on an anti-vaccine-activation tour.
Here is RFK Jr in his own words:
I went to Samoa to attend an independence celebration and discuss with the government the introduction of a medical informatics system that would allow Samoa’s health officials to assess, in real time, the efficacy and safety of every medical intervention or drug on overall health. Edwin Tamasese had arranged the trip and Children’s Health Defense had offered to finance the innovative system. Samoa banned certain vaccinations after several children had died following MMR vaccines the previous year.
While RFK Jr visited Samoa to attend an independence celebration at the invitation of the Prime Minister, he did meet (coincidentally, according to RFK Jr) with an individual who openly voiced her concerns about the safety of vaccines. Also, RFK Jr acknowledged the trip was arranged by an individual1 Edwin Tamasese. His story can be found in articles by the Brownstone Institute and RFK Jr. who was later jailed apparently for providing vitamins to the parents of Samoan children as a treatment for measles (the official charge was “incitement against a government order”; he was later released and charges against him dropped). RFK Jr had also said he and the Prime Minister talked “a limited amount” about vaccines, according to the Samoa Observer.
What was the vaccine coverage upon RFK Jr’s arrival?
Vaccination estimates for measles were 31% in 2018, as discussed in the previous section. Rates in 2019 were estimated to be nearly 90% — 87% by UNICEF & the WHO’s accounts (see Figure 3) — but this is primarily attributed to a mandatory mass vaccination campaign in November and December, including a two-day nationwide lockdown where vaccination teams went door-to-door. In the estimates for 2019, Samoa reported vaccination coverage of 96% (this is presented as the “Official” estimate in Figure 3). It noted that “catch up doses were included with routine reports during intensification activities from October to December due to a measles outbreak.” The annual estimates are the percentage of the target population who received the first dose of the MMR vaccine. In Samoa, the first MMR dose was recommended at 9 months of age. (In the US, the CDC recommends that children get the first MMR vaccine dose at ages 12 through 15 months.) The target population is the annual number of infants surviving their first year. For example, the target population used to estimate 2018 vaccine coverage includes any individual who celebrated their first birthday that year (i.e., a date of birth between January 1, 2017 and December 31, 2017).
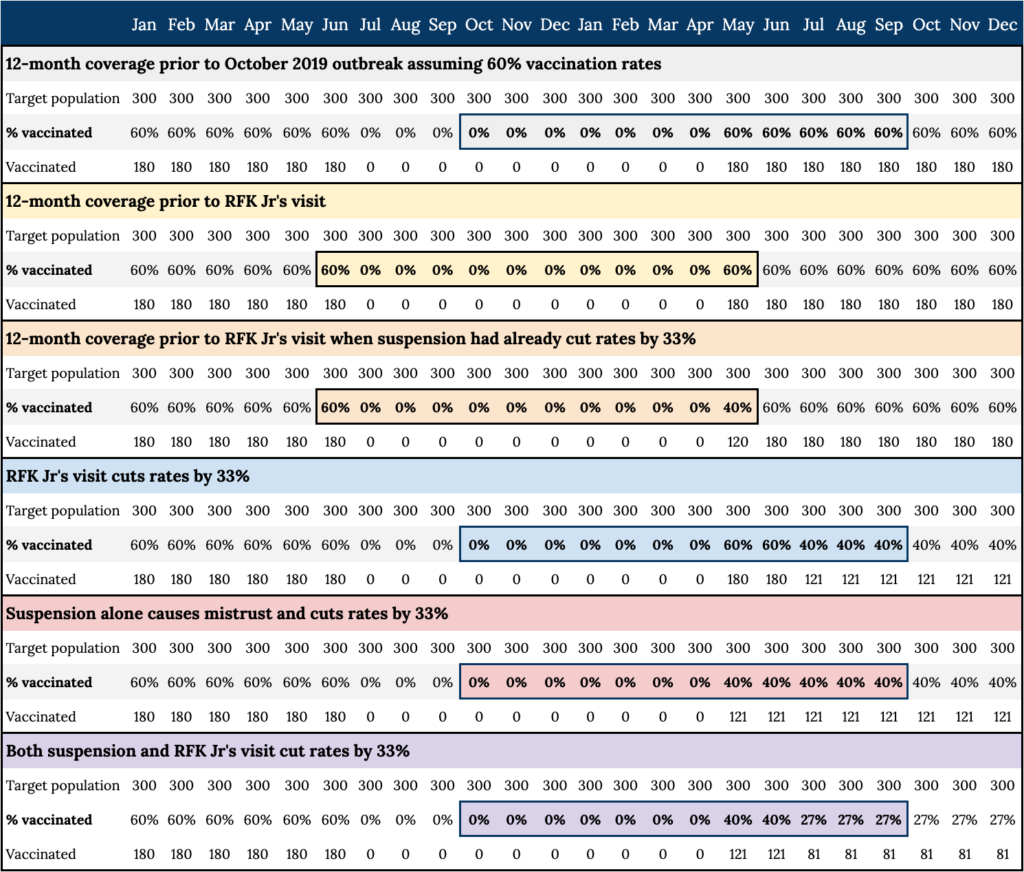
Recall that the MMR vaccination program was suspended for 10 months, from July 2018 to April 2019. Imagine that there are 3,600 infants in the target population — this shouldn’t be too far off from reality given the country’s population pyramid in 2020 — about 300 individuals in the target population each month. Based on the 2017 and 2018 estimates — 58% and 31%, respectively — and given the vaccination program was shut down in the first half of 2018, we can estimate that the monthly vaccination rate was about 60% before the infant deaths in July. All things equal, unexpectedly shutting down a vaccination program for the last six months of the year will cut annual coverage in half.
What might the 12-month vaccination rates look like upon RFK Jr’s arrival in June 2019? In the preceding 12 months, assuming 60% uptake in the entire months the vaccine was available (June 2018 and May 2019) — the estimated vaccine coverage is 10% (360 vaccinations in a target population of 3,600).2 Here’s the back of the envelope (also see Figure 4).
Did RFK Jr cause a decline in vaccination rates due to his visit?
The stories rely on RFK Jr’s supposed controversial stance on vaccines, his connection with vaccination opponents, and his visit to the country before the outbreak. Depending on the story, RFK Jr delivered an anti-vax message, gave a boost to anti-vaxxers by meeting with them, or both.
RFK Jr denies telling anyone in Samoa not to vaccinate. He acknowledged that he and the Prime Minister talked “a limited amount” about vaccines, according to the Samoa Observer.
While RFK Jr visited Samoa, he met (coincidentally, according to RFK Jr) with an individual who openly voiced her concerns about the safety of vaccines, and the trip was arranged by an individual who was later jailed apparently for providing vitamins to the parents of Samoan children as a treatment for measles (the official charge was “incitement against a government order”; he was later released and charges against him dropped). Whether this emboldened vaccination opponents and contributed to declining vaccination rates is conjecture.
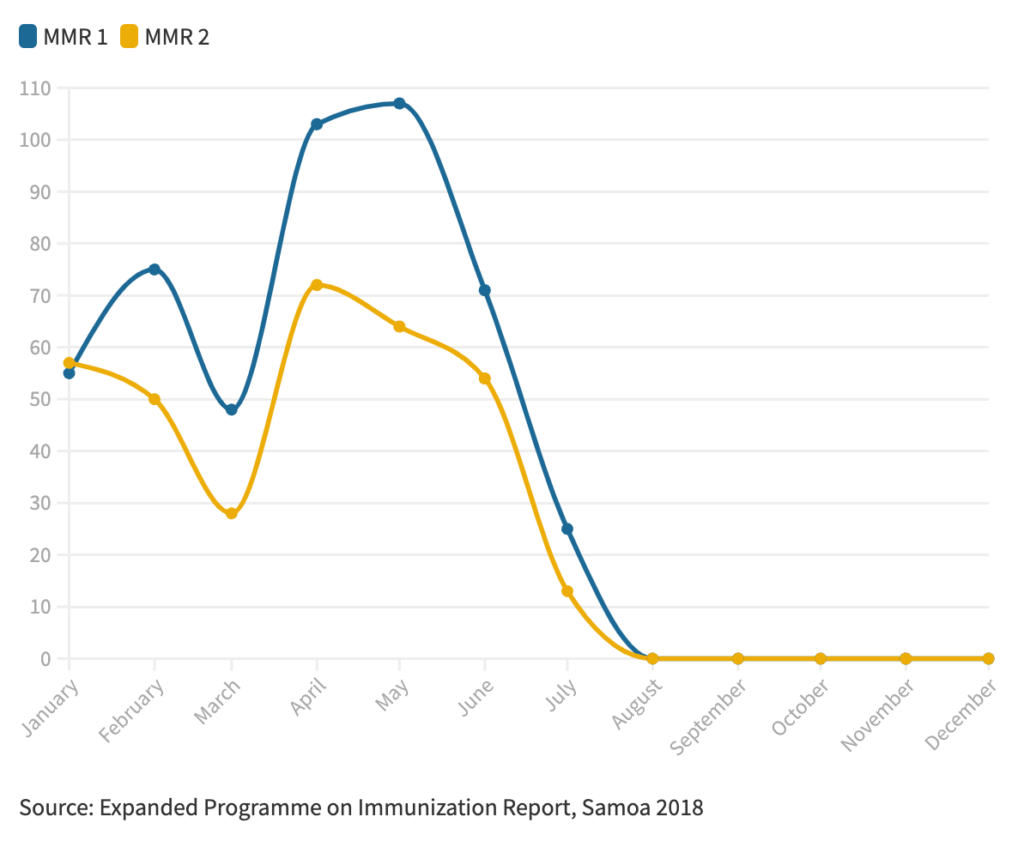
We cannot know whether RFK Jr.’s visit to Samoa contributed to a decline in vaccination rates. No data on monthly vaccination rates during this time are available. However, one reporter suggests that documents may be accessible because she presented a graphic (Figure 4 below) of monthly vaccination coverage in 2018 (”Source: Expanded Programme on Immunization Report, Samoa 2018”). Given the circumstances, why these are not available for 2019 is puzzling.
Samoa Observer (February 13, 2021):
But in the months before the infants died in the July 2018 Safotu Hospital incident, M.M.R. vaccine coverage among infants had exceeded expectations, internal hospital documents reveal.
Nevertheless, if monthly data for 2019 becomes available, we would still have no way of determining whether any association between vaccination rates after his visit can be attributed to him or myriad other factors that are also effectively unmeasurable (and some unknown).
How much influence could RFK Jr have on vaccination rates by his visit?
Recalling our previous estimates, it’s not unreasonable to assume that 12-month MMR vaccination coverage was remarkably low upon RFK Jr’s visit, in the ballpark of 10%. This is directly a result of the vaccine program being shut down for 10 of those months to investigate the deaths of two infants caused by the administration of MMR vaccines.
In response to “the incident of 6 July 2018” (the two infant deaths), “The government acted immediately to recall and suspend the MMR vaccination programme for 10 months, until it was declared safe to resume when the adverse effects were clarified,” the Ministry of Health said in their 2019 annual report (p. 14). “The incident generated a sense of mistrust in the healthcare system.” While “the incident” may have generated a sense of mistrust in the healthcare system, a 10-month suspension of the MMR vaccination program almost assuredly generates a sense of mistrust in the MMR vaccine. What is the public supposed to make of a vaccine that the government took off the shelf for nearly a year before being reintroduced? If Offit (quoted at the beginning of this article) is correct — that it was realized in less than a month that the infant deaths were due to human error and not the vaccine itself — why did it take nearly a year to exonerate the vaccine and resume the program?
The short answer may be that MoH set up a Commission of Inquiry on the incident that didn’t get started until mid-September and adjourned two days later until after the court proceedings against the two nurses charged with the manslaughter of the infants were concluded.) All of this is to say that the reaction to the incident may be worse than the incident itself (however tragic) for generating mistrust. “There was a Commission of Inquiry (COI),” the Ministry of Health acknowledges in the annual report (p. 14), “which also added to the delay in the re-launch of the vaccination programme.”
We’ve already concluded that it’s effectively unknowable whether RFK Jr’s visit contributed to a decline in vaccination rates on top of the fact there are no reported estimates of the short-term rates recently prior, during, or after his visit. Even if we assume he did lower the vaccination rates in the community, we still don’t know by how much nor what this means on an absolute basis. However, we can be reasonably confident in our estimate of 10% sometime in April or May of 2019. To be sure, there are several assumptions we glossed over, such as birth rate and infant mortality rate. But when we can be almost sure that no vaccinations were received for about 80% of our estimate and assume the 31% estimate for 2018 by UNICEF & the WHO is reasonably accurate, we should be in the neighborhood. So, we can use our estimate and at least speculate about relative and absolute differences.
On October 16, 2019, a measles outbreak was declared. So RFK Jr has about three months for any of his behavior in June to take hold — July through September. Let’s entertain the idea that RFK Jr caused a substantial decline in vaccine rates due to his visit. Let’s say he cuts the rates by a third.
Using our previous assumptions (e.g., a 60% MMR vaccination rate before the suspension and uniform uptake month over month), what happens to vaccine rates?
It’s also worth exploring what might happen if the shutdown of the vaccine program had a similar impact on vaccine rates when the program resumed compared with before the suspension.
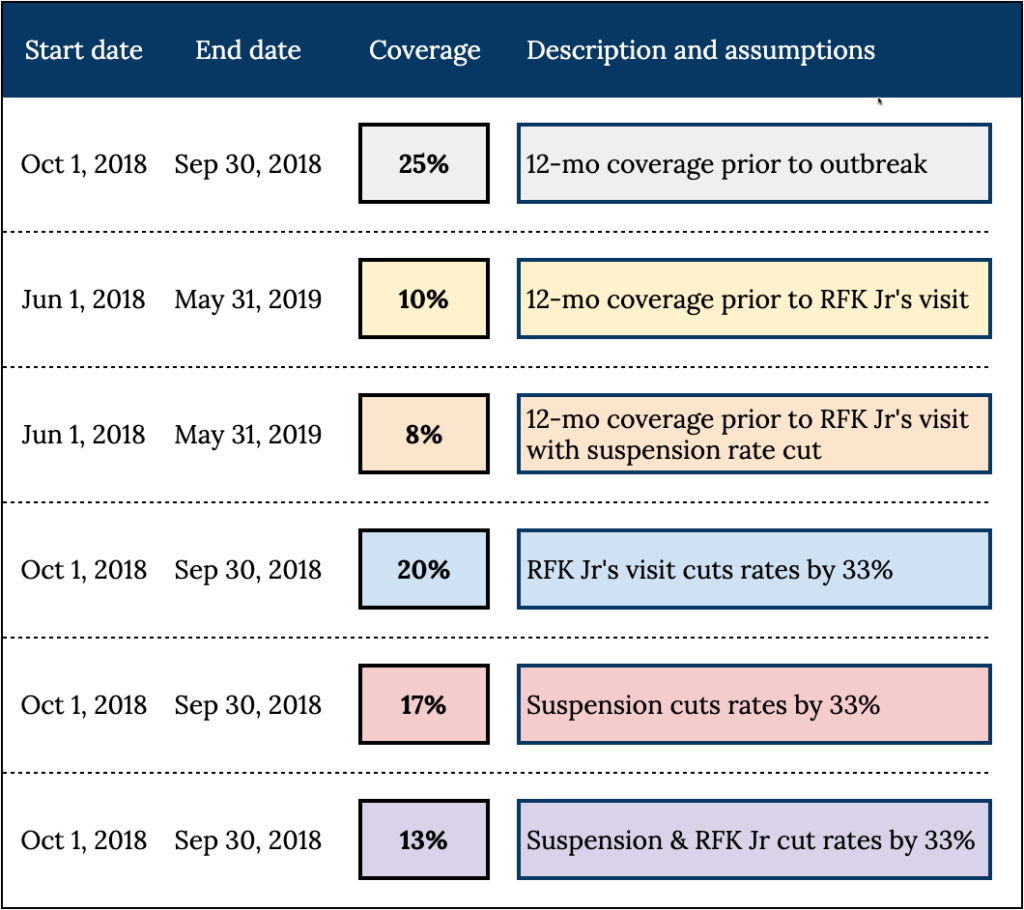
Here are four scenarios (Figure 4 shows the key dates and how the estimates were derived):
- Both RFK Jr’s visit and the suspension cut the rates by one-third (40% rate post-suspension; 27% rate post-visit)
- RFK Jr’s visit had no impact on vaccination rates, but the suspension led to a 33% decrease in vaccination rates (40% rate post-suspension)
- RFK Jr’s visit leads to a 33% decrease in vaccination rates (40% rate post-visit)
- RFK Jr’s visit has no impact on vaccination rates, and they stay the same as before the suspension (60% rate)
What do the 12-month vaccination rates look like heading into October of 2019?3 Here’s the back of the envelope (also see Figure 4).
- RFK Jr and the suspension each cut rates by one-third: 13%
- Suspension alone cut rates by one-third: 17%
- RFK Jr alone cut rates by one-third: 20%
- No change in rates: 25%
Our estimated RFK Jr baseline rate is 10% heading into June if we assume the vaccine rates picked up in May 2019, where they left off before the suspension (60%). This baseline rate drops to 8% when the suspension drops by a third because the vaccine rates are lower for a month before RFK Jr arrives. Let’s look at each scenario with our baseline (12-month rates at the end of May) and follow-up (12-month rates at the end of September) to view the vaccine coverage in context.
- If the suspension cut rates by a third (60% → 40%), and then RFK Jr comes along and cuts those rates by a third (40% → 27%), vaccine coverage would increase from 8% upon RFK Jr’s arrival in June and increases to 13% just before the measles outbreak in October.
- If the suspension cut rates by a third (60% → 40%), and RFK Jr’s visit had no impact, vaccine coverage would increase from 8% to 17%.
- If the suspension had no impact, and RFK Jr’s visit cut rates by a third (60% → 40%), vaccine coverage would increase from 10% to 20%.
- If things just picked up where they left off before the suspension of the program (60% vaccination rate), and RFK Jr’s visit had no impact, the government could expect vaccine coverage to climb from 10% post-suspension to 25% by the end of September.
Let’s address the sole impact of RFK Jr (i.e., no effect from the suspension on vaccine rates) in our hypothetical scenario #3. Even though RFK Jr’s visit indeed caused vaccine rates to drop by a third — from a rate of 60% to 40% — what we observe is that vaccine coverage increases by (i.e., 10% to 20%) between the time he visited and the declaration of a measles outbreak. If this is all we know, we might conclude that RFK Jr’s visit caused MMR vaccine coverage to double before the measles outbreak. But that’s not all we know. To estimate the baseline and follow-up coverage, we need to consider the suspension of the vaccine program from July 2018 to April 2019. The preceding 12 months from baseline includes roughly a 10-month period (July-April) when the program was suspended, whereas the follow-up included seven (October-April).
We have no idea whether RFK Jr’s visit impacted vaccination rates or how much. On the other hand, we do have a good idea of whether seizing the vaccine supply and shutting down the program impacts vaccination and by how much, or at least we should.
One important caveat in these estimates is that they do not account for any catch-up doses. Catch-up doses are vaccinations given to children who did not receive it at the recommended age. There were a lot of children that fit this description coming out of the suspension of the MMR program. However, the vaccine coverage report from UNICEF & the WHO explains the Samoan government told them that catch-up doses occurred from October to December (as noted above) — after they declared a measles outbreak.
To avoid significant measles outbreaks, the target population vaccination rate is typically estimated to be around 95%. If we assume this to be accurate and that low vaccination rates caused the measles outbreak, the Samoan government had already done the damage. Suppose people want to blame the measles outbreak on anti-vaxxers, increasing parent mistrust and, therefore, lower vaccine coverage. In that case, they should also explain why they believe 20% vs 10% coverage makes the difference between a protected community and a measles outbreak.
Government influence on low vaccination coverage
Recall that the Ministry of Health was waiting on the Commission of Inquiry before they could resume the vaccination program, adding to the delay, according to the Ministry. It turns out that the Commission submitted its final report on March 29, 2019, and recommended the immediate implementation of a mass vaccination campaign.
According to an article in the Samoa Observer:
The Government ignored advice from its own Commission of Inquiry to roll out a national measles vaccination campaign six months before an outbreak of the disease claimed 83 mostly infant lives.
The commission’s final report, obtained by the Samoa Observer, shows the Government was warned a global measles epidemic was edging closer to Samoa day-by-day.
The Recommendations section of the COI report can be found here (uploaded by the Samoa Observer reporter to Scribd). The reporter also revealed that a separate Ministry of Health review into its national vaccine programme in 2018 made the same recommendation. “Lift the ban on MMR introduction and resume before it is too late. The 0% on MMR coverage alarms and flashes a red signal of loosing [sic] our children tomorrow,” the review states (Figure 5).
The Recommendations section of the COI report can be found here (uploaded by the Samoa Observer reporter to Scribd). The reporter also revealed that a separate Ministry of Health review into its national vaccine programme in 2018 made the same recommendation. “Lift the ban on MMR introduction and resume before it is too late. The 0% on MMR coverage alarms and flashes a red signal of loosing [sic] our children tomorrow,” the review states (Figure 5).
Additionally, an assessment by the United Nations concluded that the measles outbreak resulted from the vaccination program’s suspension and vulnerabilities in Samoa’s healthcare system.
The following is from a statement (p. 3) by the UN Resident/Humanitarian Coordinator Simona Marinescu:
The 2019 measles outbreak in Samoa was the result of the interruption of MMR vaccination for close to 9 months after the immunization incident in July 2018 that led to the death of two babies. Despite continued efforts by WHO and UNICEF, routine vaccination remains suboptimal in Samoa and across the Pacific. The increase of measles cases in October 2019 found the health system of Samoa unprepared to respond and the population across islands unaware of the potentially devastating consequences of the MMR epidemic.
Here’s the Samoa Observer (December 8, 2019) reporting:
The United Nations has contradicted the Samoan Government’s explanation for the causes of the measles outbreak, saying that a lack of access to immunisation and public education campaigns helped create the conditions for the epidemic.
Despite what the U.N is calling an “honest assessment” of Samoa’s vulnerabilities being released to the world in a joint response appeal for nearly $30 million, Prime Minister Tuilaepa Dr. Sailele Malielegaoi is insistent that anti-vaccination lobbyists and parents are responsible.
“The vulnerabilities have been recognised by this government in this document, this document is informed by the government,” U.N Resident Coordinator Simona Marinescu said at the appeal launch on Friday.
The “NATIONAL MEASLES RESPONSE AND RECOVERY APPEAL” document (December 6, 2019) can be found here.
It wasn’t until June 18, 2019, when a team of New Zealand nurses arrived in Samoa for a 10-day mission to re-train all vaccinating nurses. This comes one year after the two nurses mixed the wrong liquid with the MMR vaccine, causing the deaths of two infants.
In July, a report by the WHO’s Global Advisory Committee on Vaccine Safety observed that initial attempts to hide the vaccination error, poor communication, and blaming individuals rather than conducting systemic analyses had a detrimental effect on the vaccine program. “Because of this,” explained infectious disease epidemiologists in the Lancet, “rumours began to circulate in the community about the lack of safety of vaccines, and after the restart of the vaccination programme previously high coverage was not achieved for all vaccines on the National Immunisation Programme.”
Claim 2 | Conclusions
Critics allege that RFK Jr’s June 2019 visit to Samoa reduced vaccination rates by supporting local vaccine opponents and fostering mistrust. However, the evidence linking his visit to declining vaccination rates is speculative and overshadowed by systemic factors.
By June 2019, vaccination rates were already very low due to the 10-month suspension of the MMR program. While RFK Jr’s visit coincided with ongoing public mistrust, no data supports the claim that his presence significantly influenced vaccination rates. The broader systemic failures in public health communication and infrastructure remain more plausible explanations for the low vaccine uptake preceding the outbreak.
There is no evidence that RFK Jr’s visit significantly influenced vaccination rates. Systemic failures and delays in public health interventions primarily drove the low vaccination rates.
Claim 3 | In his letter to the Samoan Prime Minister, RFK Jr deflected blame from the anti-vaccine movement and instead spread misinformation by suggesting the outbreak was caused by a defective vaccine
Claim 3 | Synopsis
Critics argue that RFK Jr’s November 2019 letter to the Samoan Prime Minister deflected blame from the anti-vaccine movement by suggesting the outbreak was caused by a defective vaccine. However, this claim ignores the broader systemic issues that contributed to the outbreak.
RFK Jr’s letter raised legitimate scientific questions about potential causes of the outbreak, including vaccine-derived disease and maternal immunity. While critics viewed this as misinformation, his letter also emphasized the importance of a thorough investigation into the outbreak’s etiology.
The 10-month suspension of the MMR program and systemic healthcare vulnerabilities were the primary drivers of low vaccination rates. RFK Jr’s letter sought to explore alternative explanations for the outbreak, which could inform future public health strategies. Criticizing systemic failures directly in a letter to the Prime Minister would likely have been counterproductive.
RFK Jr’s letter did not deflect blame but rather raised important scientific questions. The systemic failures in Samoa’s healthcare system remain the primary contributors to the outbreak.
Claim 3 | Introduction
When the Samoan government declared a measles outbreak on October 16, 2019, there had been one associated death. By October 30, there were three related deaths.
On November 15, a State of Emergency was declared, with 16 associated deaths at this point. By November 29, 42 related deaths.
On November 19, RFK Jr sent the Samoan Prime Minister a letter. “To safeguard public health during the current infection and in the future,” he wrote, “it is critical that the Samoan Health Ministry determine, scientifically, if the outbreak was caused by inadequate vaccine coverage or alternatively, by a defective vaccine.”
RFK Jr outlined three alternative hypotheses in the form of the following three questions that Samoan Health Officials must answer to determine the cause of the outbreak:
- What were the ages of the victims? Stated differently: Did the vaccine fail to produce antibodies in the vaccinated mothers sufficient to provide the infant with maternal immunity?
- Were Samoa’s fatal measles cases caused by strains of measles not targeted by Merck’s vaccine?
- Were the fatal Samoan infections from a vaccine strain?
Several news outlets reported on this letter, branding it as more anti-vaccine misinformation from RFK Jr. According to these stories, RFK Jr is promoting vaccine hesitancy during the outbreak or attempting to deflect blame from the anti-vaccine movement.
Here’s how the WaPo recently reported it (November 15, 2024):
Robert F. Kennedy Jr., the health secretary nominee widely known for his anti-vaccine views, questioned whether problems with the measles vaccine caused the Samoan outbreak, rather than insufficient vaccine coverage. Kennedy’s own family members have said he is spreading dangerous misinformation about vaccine doses.
The Children’s Health Defense, Kennedy’s advocacy group, did not immediately reply to a question sent late Thursday about whether he still opposes measles vaccination.
Here’s Ars Technica reporting, weeks after the letter was sent (December 2, 2019):
In November, Kennedy’s organization sent a letter to the Samoan prime minister, encouraging officials to question the MMR vaccine. Kennedy peddles the false and dangerous claim that vaccines are linked to autism, despite the fact that numerous scientific studies have robustly debunked the baseless claim.
On Sunday, Samoan Prime Minister Tuilaepa Sailele Malielegaoi encouraged residents to fight back against misinformation. “Let us work together to encourage and convince those that do not believe that vaccinations are the only answer to the epidemic,” he said.
Is RFK Jr attempting to deflect blame from the anti-vaccine movement for the measles outbreak?
Here’s TIME reporting in 2023:
Despite the deadly outbreak, Kennedy wrote a letter to Samoa’s Prime Minister Malielegaoi to deflect blame from the anti-vaccine movement and instead suggest that the outbreak was due to a defective MMR vaccine.
The reporter is probably referring to a statement from RFK Jr in opening his letter to the Prime Minister.
I was dismayed—but not surprised—to see media reports that linked the current measles outbreak to the so-called “anti-vaccine” movement. While we can expect pundits to engage in uninformed finger-pointing, Samoa’s public health officials must undertake the serious tasks of containing the infection and—equally importantly—to thoroughly understand its etiology. To safeguard public health during the current infection in and in the future, it is critical that the Samoan Health Ministry determine, scientifically, if the outbreak was caused by inadequate vaccine coverage or alternatively, by a defective vaccine.
Is this an attempt to deflect blame from the anti-vaccine movement for the measles outbreak by suggesting the outbreak was due to a defective MMR vaccine?
By stating it this way, the reporter implicitly lays blame on the anti-vaccine movement for inadequate vaccine coverage leading up to the outbreak.
However, as discussed in the previous sections, the 10-month suspension of the MMR vaccination program between July 2018 and April 2019 is to blame for the poor vaccine coverage. Any observer — or at least one who does not faithfully accept explanations from public health institutions — understands this. RFK Jr. is no exception.
Recall that UNICEF asserts, “…vaccination coverage in Samoa plummeted from 58 per cent in 2017 to just 31 per cent in 2018, largely due to misinformation and mistrust among parents.” The Prime Minister of Samoa insists the same thing.
However, common sense, and the United Nations, for that matter, disagree.
Here’s the Samoa Observer (December 8, 2019) reporting:
The United Nations has contradicted the Samoan Government’s explanation for the causes of the measles outbreak, saying that a lack of access to immunisation and public education campaigns helped create the conditions for the epidemic.
Despite what the U.N is calling an “honest assessment” of Samoa’s vulnerabilities being released to the world in a joint response appeal for nearly $30 million, Prime Minister Tuilaepa Dr. Sailele Malielegaoi is insistent that anti-vaccination lobbyists and parents are responsible.
So this isn’t just an issue about inadequate vaccine coverage vs a defective vaccine. It’s also an issue about whether the so-called anti-vaccination movement or the Samoan government caused the inadequate vaccine coverage. As previously discussed, we and others — including Samoa’s UN Resident Coordinator — argue that the latter is responsible for the low vaccine coverage. In other words, the finger points to the Samoan healthcare system, which is not constructive for RFK Jr to make in a letter to the country’s Prime Minister when the letter intends to help Samoa investigate alternative explanations for the etiology of the outbreak.
There were also problems during the outbreak. On November 4, 2019, the Samoan Observer reported that patients seeking MMR vaccinations were turned away and that hospitals were struggling to keep up with demand. Despite this, the Ministry of Health repeatedly declined to respond publicly.
On November 19, the Samoa Red Cross Society had to turn away about 200 people seeking vaccinations after the Ministry of Health said their mass vaccination program was not yet finalized.
On November 23, the Government of Samoa informed the public that private clinics providing measles vaccinations for a fee had been shut down as inquiries were proceeding: “The Ministry of Health wishes to clarify that currently there is no formal agreement between private clinics and the Ministry on the operations and safety requirements needed for maintaining the quality of the vaccines,” the Director General said. It was not clear to the Ministry of Health how the vaccines, which could have only been obtained by the government, were made available to these clinics.
Only two days later, RNZ reported that the Director General said a second private clinic that provided vaccination had done so after being approved by the previous National Health Services and was awaiting re-evaluation by UNICEF and the Ministry of Health to restart the administration of measles vaccination. “Ten facilities besides district health centres were listed as providing vaccinations and treatment for measles (Government of Samoa 2019a), but this information was only made public a few days before the mobile outreach campaign commenced,” according to a 2020 review by Penelope Schoeffel and her colleagues. Until that happened, most people were expected to travel to health centers on both major islands, the Samoa Observer reported.
“The rapid spread was clearly related to the delay in declaring an outbreak and building public awareness and the confusing response by the Ministry of Health,” according to Shoeffel et al.’s (2020) review. “Despite advice from the World Health Organisation and UNICEF, Samoa was not prepared for the epidemic.”
Did vulnerabilities in Samoa’s healthcare system contribute to higher mortality rates?
The 2020 review by Schoeffel and colleagues also indicates that substandard care may have contributed to the high case fatality rates during the outbreak.
Media reports highlight instances where children were sent home with fever medication. One report described a seven-month-old with fever and refusal to feed who was turned away five times before being admitted and treated for measles; the mother stated she was labeled a “paranoid mum.” In a separate incident, a child who was twice misdiagnosed with the common cold later succumbed to complications of measles. The child had missed the first MMR vaccine appointment due to the suspension of the vaccination program in 2018. A further tragic case involved a child (known to one of the authors of the 2020 review) in remission from cancer who was called to the hospital for a checkup. Being immunosuppressed, he contracted measles and passed away about a week later. A reporter from the Samoa Observer exposed severe shortages of health workers, essential equipment, and inadequate training on Samoa’s measles treatment protocol, emphasizing the deficiencies in the hospital’s response to the outbreak. The district health facilities, which collectively have a total bed capacity of only 80 across eight locations (with no single facility exceeding 15 beds), were overwhelmed during the outbreak. Approximately 42% of referred cases at emergency departments originated from district facilities, underscoring their inability to manage the crisis.
Systemic dysfunction within the health system contributed to a delayed and chaotic response during the early stages of the outbreak, according to the 2020 review. As the infection spread and the death toll rose, many fearful and confused members of the public resorted to ineffective traditional and alternative treatments.
The data indicate a measles case fatality rate (CFR) of about 146 deaths per 10,000 cases (83 deaths out of 5,700 reported cases) or about 1.5%.
In contrast, a 1994 report by the Institute of Medicine indicates that in developed countries like the US, “the measles fatality rate is 1 per 10,000 cases,” a CFR of 0.01%. The CDC reports that in the US, for every 1,000 children who get measles, one or two will die from it, yielding a case fatality rate of 10-20 per 10,000 cases.
The differences in estimates between the IOM and CDC are likely due to the use of estimated cases and reported cases in the denominator, respectively. (The CDC also reports an estimated 3-4 million cases in the same citation compared with 500,000 reported cases, yielding a CFR of 1-2 per 10,000 cases, the same as the IOM’s estimate.)
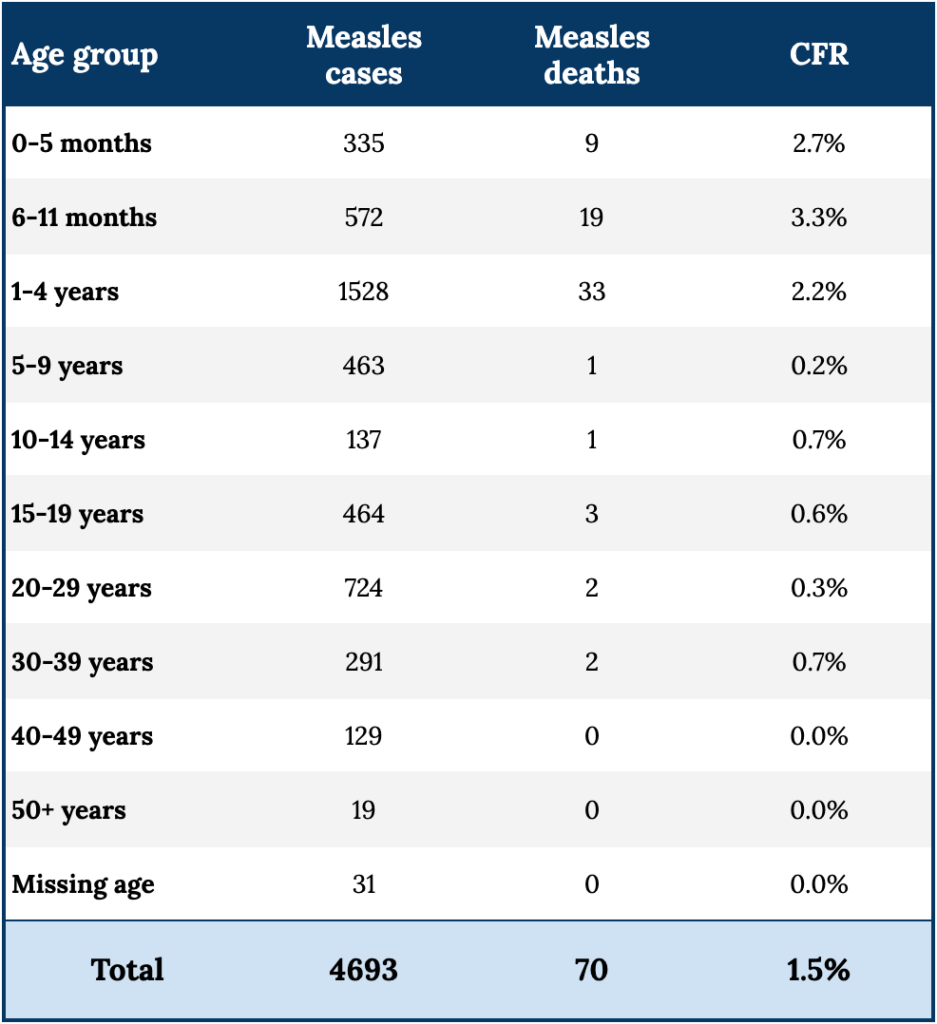
Nevertheless, the case fatality rate in Samoa appears to be at least 10 times higher than rates reported in the US. Not only that, but death rate in children younger than 12 months was 28 deaths out of 907 cases — a CFR of 3% (also see Figure 6, below).
Recall RFK Jr’s first question to the Prime Minister: What were the ages of the victims?
“Media reports from Samoa suggest that the infection is targeting young infants who are not yet of age to receive the measles vaccine,” RFK Jr noted. “If true, the culprit is most likely a vaccine that failed to produce antibodies in the vaccinated mothers sufficient to provide the infant with maternal immunity.”
While a determination of the plausibility of RFK Jr’s alternative hypotheses is beyond the scope of this investigation, to see such a stark difference in mortality rates in Samoa compared with Westernized nations as well as surrounding populations that concurrently reported measles outbreaks with much lower fatality rates, this observation suggests that something other than low vaccination rates increased the severity of the disease in Samoa.
Besides inadequate coverage or a defective vaccine, additional factors can contribute to measles complications. This disease in 1962 was described as a “self-limiting infection of short duration, moderate severity, and low fatality.” Two important factors are nutritional status and access to and quality of medical care.
Data from UNICEF and the Food and Agriculture Organization indicate vitamin A deficiencies in Samoan children. Vitamin A deficiency is a recognized risk factor for severe measles, and the WHO reports that a low vitamin A status can significantly worsen measles outcomes, leading to increased complications and mortality, and therefore recommends providing vitamin A supplementation to all children diagnosed with measles. It probably also didn’t help matters that Tamasese promoted its use and helped supply citizens with vitamin A because vitamin A supplementation was now branded and promulgated by the media as an ineffective treatment peddled by anti-vaxxer conspiracy theorists.
The evidence suggests that iatrogenesis (i.e., harm experienced by patients resulting from medical care), limitations within the healthcare system, or both contributed to higher measles mortality rates in Samoa.
Claim 3 | Conclusions
The criticism that RFK Jr’s letter deflected blame from the anti-vaccine movement overlooks the fact that the low vaccine coverage was primarily caused by the Samoan government’s suspension of the MMR program, not misinformation. Blaming the anti-vaccine movement for inadequate coverage ignores the systemic issues leading to the outbreak.
Rather than deflecting blame, RFK Jr’s letter sought to assist Samoa in investigating the causes of the outbreak, highlighting legitimate scientific concerns such as vaccine efficacy, vaccine-derived disease, and maternal immunity. While critics view this as an attempt to undermine public health efforts, the questions raised are essential to guide effective public health strategies. Pointing out failures in Samoa’s healthcare system in a letter to its Prime Minister would likely have been unproductive. Instead, the letter focused on actionable steps to identify and address the outbreak’s root causes.
Closing
The suspension of the MMR program following the deaths of two infants in 2018 drove the reduced vaccination rates, not misinformation or external influences. While RFK Jr’s actions and statements may have drawn attention to vaccine safety issues, their impact on Samoa’s vaccination rates remains speculative. Raising awareness about legitimate vaccine safety concerns is vital in ensuring informed consent and accountability in healthcare. Public health authorities sometimes obscure, deny, or minimize legitimate safety issues to avoid potential declines in vaccine uptake. While the intention may be to protect public health, this approach can erode trust when individuals learn this information is being withheld or dismissed.
Addressing vaccine hesitancy requires acknowledging and confronting legitimate safety concerns. In some cases, hesitancy may lead to overestimating risk and rejecting a vaccine where the benefits outweigh the harms. In other cases, a cautious approach may reflect a valid risk-benefit analysis. Accurate risk-benefit analyses, however, are only feasible when there is complete transparency about potential risks and benefits, supported by data from rigorous, long-term clinical trials that are thoroughly conducted and openly reported. Public health strategies should respect this nuance and avoid dismissing or marginalizing legitimate concerns, as this violates scientific standards, can distort risk-benefit assessment, compromise safety for some individuals, and undermine trust in the long term.
Ultimately, the Samoan government’s nearly year-long suspension of the MMR vaccination program, disregard of mass vaccination advice from its medical experts in consecutive reports, poor communication with the public about the infant deaths following MMR vaccinations, and vulnerabilities in Samoa’s healthcare system caused the low coverage that preceded the outbreak.

Notes On The Issue
[1] Edwin Tamasese. His story can be found in articles by the Brownstone Institute and RFK Jr.
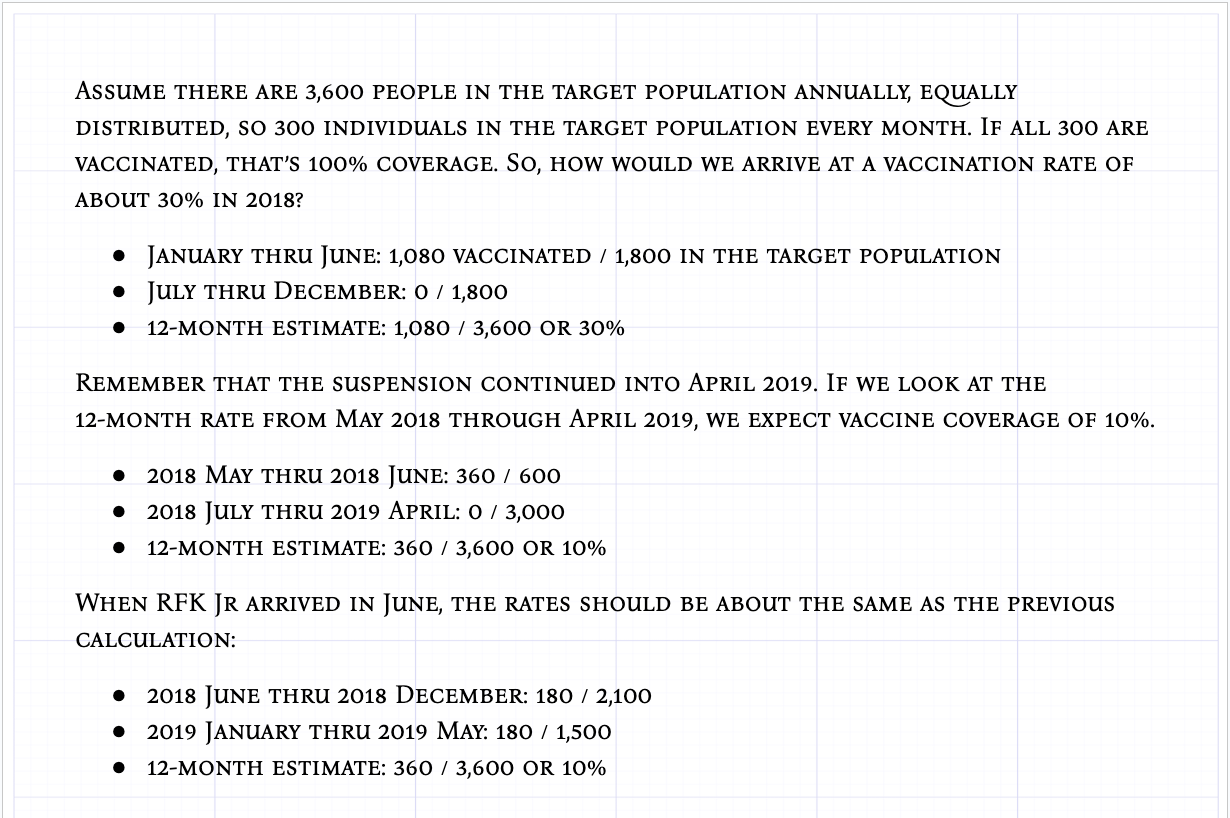
[2] Here’s the math (also refer to Figure 4). Assume there are 3,600 people in the target population on an annual basis. This is equally distributed so that there are 300 individuals in the target population every month. If all 300 are vaccinated, that’s 100% coverage. So, how would we arrive at a vaccination rate of about 30% in 2018?
- January through June: 1,080 vaccinated / 1,800 in the target population
- July thru December: 0 / 1,800
- 12-month estimate: 1,080 / 3,600 or 30%
Remember that the suspension continued into April of 2019. If we look at the 12-month rate coming out of the suspension — from May 2018 through April 2019 — we would expect vaccine coverage of 10%.
- 2018 May thru 2018 June: 360 / 600
- 2018 July thru 2019 April: 0 / 3,000
- 12-month estimate: 360 / 3,600 or 10%
When RFK Jr arrived in June, the rates should be about the same as the previous calculation:
- 2018 June thru 2018 December: 180 / 2,100
- 2019 January thru 2019 May: 180 / 1,500
- 12-month estimate: 360 / 3,600 or 10%
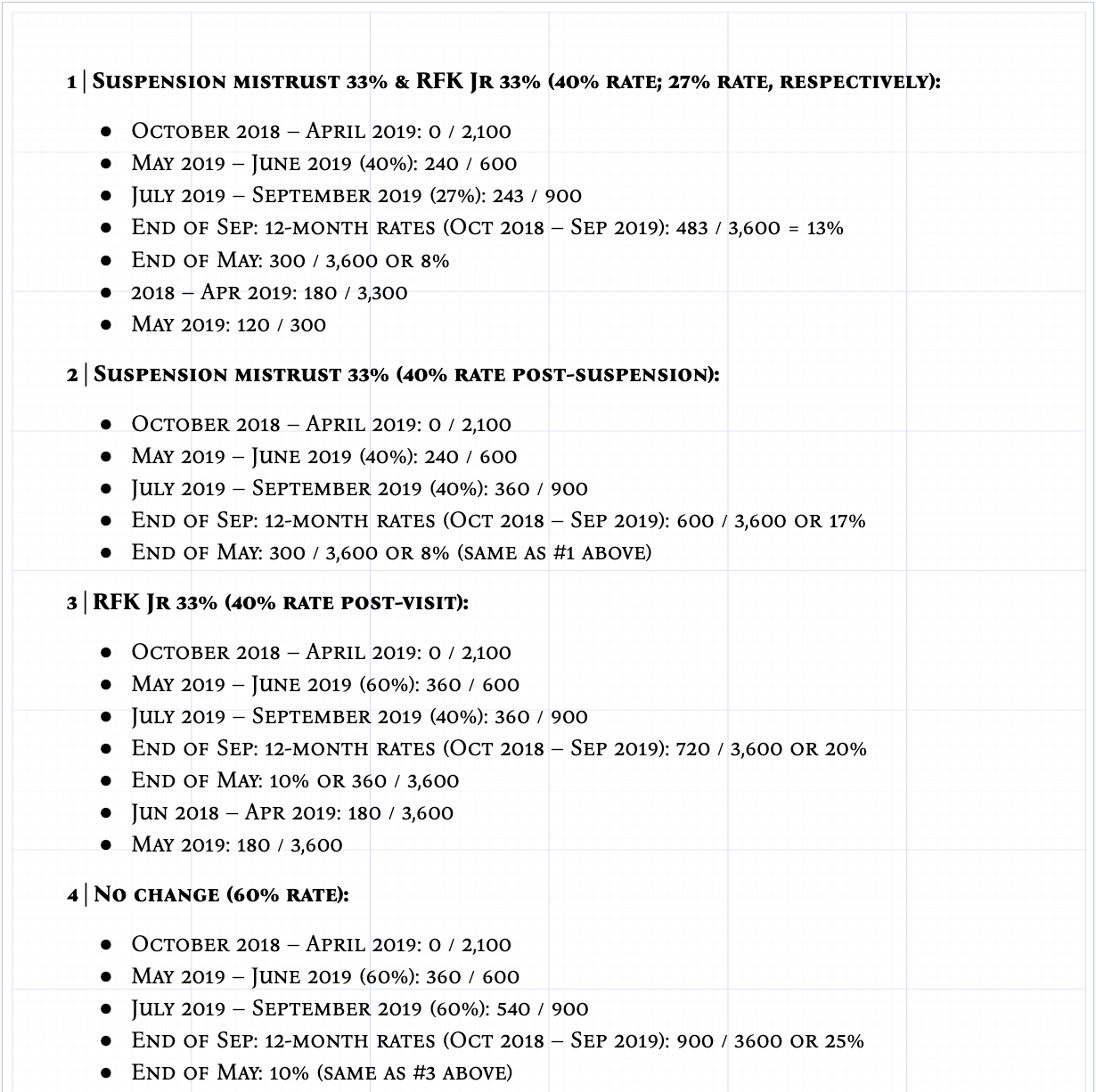
[3] Here’s the math (also refer to Figure 4):
1 Suspension mistrust 33% & RFK Jr 33% (40% rate post-suspension; 27% rate post-visit):
- October 2018 – April 2019: 0 / 2,100
- May 2019 – June 2019 (40%): 240 / 600
- July 2019 – September 2019 (27%): 243 / 900
- End of SEP: 12-month rates (October 2018 – September 2019: 483 / 3,600 = 13%
- End of MAY: 300 / 3,600 or 8%
- 2018 – Apr 2019: 180 / 3,300
- May 2019: 120 / 300
2 Suspension mistrust 33% (40% rate post-suspension):
- October 2018 – April 2019: 0 / 2,100
- May 2019 – June 2019 (40%): 240 / 600
- July 2019 – September 2019 (40%): 360 / 900
- End of SEP: 12-month rates (October 2018 – September 2019: 600 / 3,600 or 17%
- End of MAY: 300 / 3,600 or 8% (same as #1 above)
3 RFK Jr 33% (40% rate post-visit):
- October 2018 – April 2019: 0 / 2,100
- May 2019 – June 2019 (60%): 360 / 600
- July 2019 – September 2019 (40%): 360 / 900
- End of SEP: 12-month rates (October 2018 – September 2019: 720 / 3,600 or 20%
- End of MAY: 10% or 360 / 3,600
- Jun 2018 – Apr 2019: 180 / 3,600
- May 2019: 180 / 3,600
4 No change (60% rate):
- October 2018 – April 2019: 0 / 2,100
- May 2019 – June 2019 (60%): 360 / 600
- July 2019 – September 2019 (60%): 540 / 900
- End of SEP: 12-month rates (October 2018 – September 2019): 900 / 3600 or 25%
- End of MAY: 10% (same as #3 above)
Related News Publications

RFK Jr. appears before Congress as his comments spreading misinformation draw scrutiny




Samoa measles outbreak: WHO blames anti-vaccine scare as death toll hits 39





Measles outbreak spurred by anti-vaxxers shuts down Samoan government




{kind=link}
{kind=link}
{kind=link}
{kind=link}