
What barbell exercise is the most important for the aged? The answer really depends on who you ask or from which source of information you derive your answer.
While you see clickbait articles and videos abounding on the internet, they, as a whole, are simply content parroting someone else’s opinion that previously received a lot of reads or views. Everyone wants to ride a wave of popularity and maybe make a few bucks from their outputs, so being a content creator that copies an idea before others do so is a fairly smart thing to do, in terms of generating views and potential revenues. BUT is anyone actually doing due diligence on the veracity of the original content?
First things first; let’s actually look at what experimental data has to say about strength loss as we age. We are specifically speaking about strength loss in those of us that are essentially sedentary; the roughly two thirds of us who either do not exercise or do not do enough exercise or physical activity to produce any fitness or health benefit. Because of the overwhelming inactivity of lifestyle there is no biological stimulus to maintain muscle mass and function over time. That means we get weaker as we age, it’s an absolute if we remain sedentary. Strength loss has horrible outcomes. A twenty five percent loss of strength from that present in a healthy twenty year old is associated with the onset of clinical frailty and physical limitations. A forty five percent loss generally marks the advent of dependency on others for normal life activities and is often accompanied by institutionalization in care facilities.
So strength training must be a core recommendation for every aging person. We don’t want to be frail or dependent. But how would we select which exercise is of most utility in fighting off frailty and dependence?
The approach here is simple; assess which regions of muscular anatomy lose strength the fastest. Logic would suggest that we should pay particular and first attention to the muscles or muscle groups that fade first. The following graphic condenses and presents data from fourteen research papers (see reference section) to demonstrate differences in regional strength decay over the life span. The strength data for 20 year olds (normal people, not athletes or competitors) is considered our 100% strength level and data for every decade that follows is presented as a percent of that initial strength level. It is interesting to note that even in the untrained and sedentary populations described by the data, overall strength level increased to 105% at 30 years of age and remained fairly high, 95%, at age 50. Frailty criteria generally are not met until about age 65.
When we break whole body strength down into regions (hand, elbow, shoulder, back, and leg) there are differences in the rate of decay:
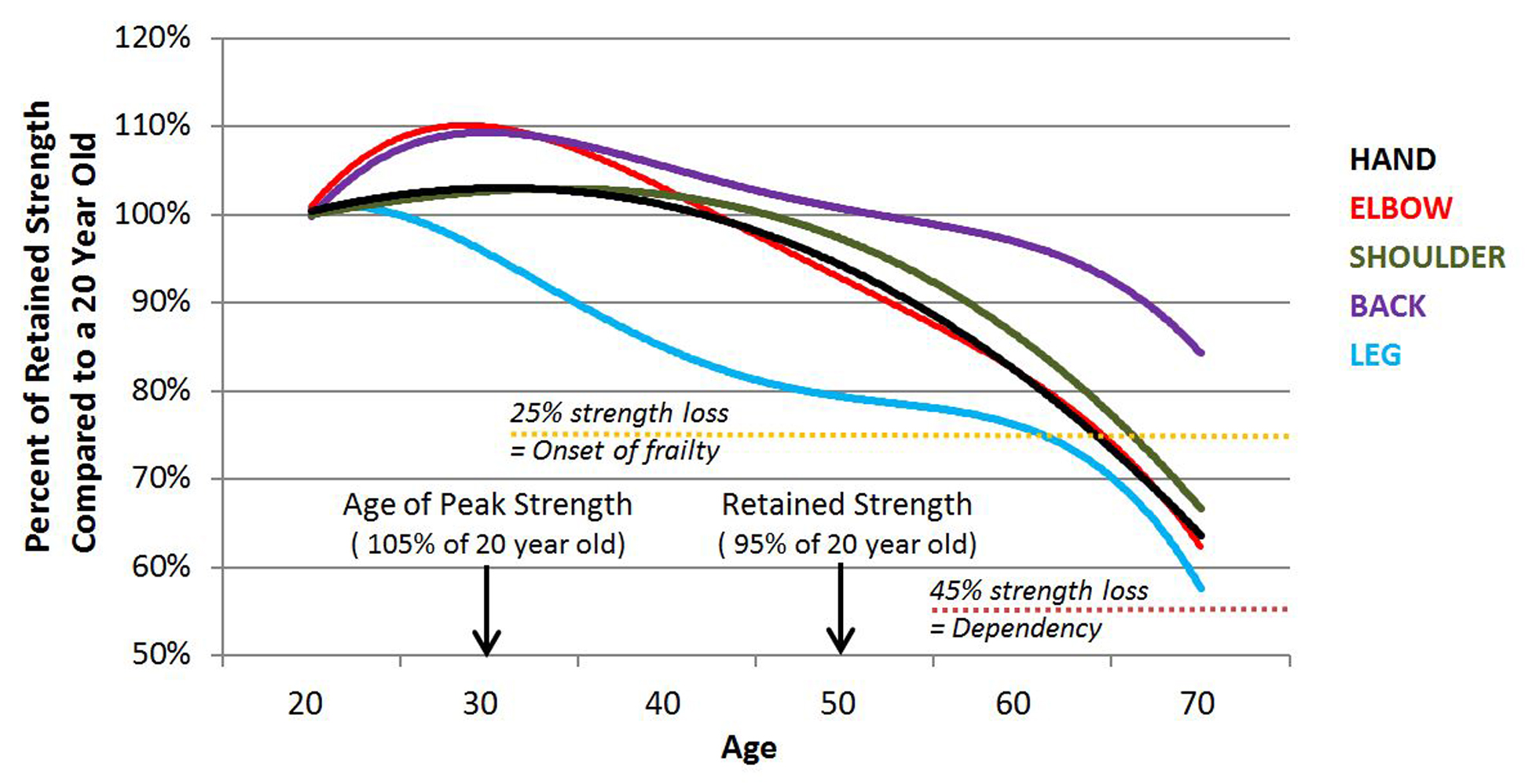
The fourteen papers that the data for the above graph was adapted from used wildly different measures and/or methods in determining and reporting strength. The data in those papers is not presented in a manner understandable within the context of how one would express strength in a gym. Very few provided real-world data such as a very simple “x kilograms were moved through the range of motion or held isometrically”. Rather, the researchers used isometric or isokinetic dynamometers (barbells and weight machines in gyms are isotonic) to produce measurement outputs in isometric kilogram force, isometric pounds force, Newton-meters, Newton-decimeters, torque in Newton-meters, or Watts. To enable use of data from all fourteen studies, the original data and any changes in magnitude over the lifespan were converted to percentages referent to the strength results of a 20 year old.
When you look at this graph two things should be quite obvious. First, the legs lose strength very quickly, beginning in the twenties, approaching frailty criteria as we approach 60 and nearing dependency levels by age 70. Second, the back is quite resilient, with strength levels not dipping below youthful strength until the mid-fifties and never appears to diminish to frail levels. Given the high incidence of back “problems” in aging populations this seems non-intuitive. However, in modernity most employment and sedentary recreation requires the engagement of hands, elbows, and shoulders. These are all anatomically supported by the back, so it really should not be surprising that it retains more function longer.
Skipping leg day and pain
So why are the legs the most affected region of the anatomy? There are a number of reasons; we drive instead of walking, we use devices to lift and labor at work rather than using muscular force, we sit because we have built our home, work, and recreational environments to enable it, and because walking – when we do walk – is such a low effort activity, there is no stimulus to keep our youthful muscle mass. Over two thirds of the population also do no exercise or physical activity or do so little of it that it has no effect. This means that if there is no leg work beyond casual and short distance/duration walking at actual work and in daily life AND there is no home based or gym based leg exercises done regularly, then leg muscles adapt by losing fitness. They get smaller, weaker, and less enduring.
How profound is this problem of leg strength loss in terms of real world ramifications? By age 55 approximately one in six Americans cannot take more than 600 to 700 steps along level ground (or one quarter mile or 440 yards) and that number increases to six out of ten being unable to do so by 85 years of age (Schoenborn et al, National Health Statistics Report 16:1-31,2009). Remember, walking is an anatomically advantageous movement requiring low levels of muscular effort, which means that a physical limitation in walking is a strong bellwether of more severe limitations in more strenuous leg dominant tasks. It is relevant to consider a recently developed clinical screening test for those over age 55 where if an individual cannot go from standing to sitting on the floor and then return to standing without using the hands or any other aid, they are at increased risk of dying within the ensuing five years (de Brito et al, European Journal of Preventive Cardiology 21(7): 892-898, 2014). Using leg strength and mobility as an indicator of possible premature death in the elderly underscores the importance of exercising to maintain or increase strength in the lower body.
But there is a problem of misperception and misunderstanding with this observation. If we look at the frequency of back and knee pain in the untrained public we find a significant frequency of pain in average, sedentary populations. Back pain reports are very common (Hoy et al, Arthritis & Rheumatology 64(6): 2028-2037, 2012) but exercise reduces its frequency and severity more than pharmaceuticals (Steffens et al, JAMA Internal Medicine 176(2): 199-208, 2016). Similarly, knee pain is also common BUT its severity is reduced with exercise (Anwer et al, Journal of Geriatric Physical Therapy 39(1): 38-48, 2016). Additionally, when a person perceives pain under specific conditions, their default belief and action is to avoid those circumstances that they believe are, or might be, associated with stimulating pain (van Vliet et al, Journal of Pain Pii S1526-5900(18): 30185-30188, 2018). So human nature, and conventional exercise wisdom, has people with back or knee pain avoiding exercising those anatomical regions. But, doing so exacerbates the condition underlying the pain and a spiral into more pain and increasing physical limitation occurs over time. This suggests that the elderly should be encouraged to exercise these pain affected areas – cautiously and with qualified oversight – in order to improve regional strength, reduce perceived pain, and maintain lifelong physical function.
Dialing in an exercise recommendation
So, the answer to which exercise is the most important in aging is fairly clear, and it is an exercise that should be done throughout the complete lifespan. If leg strength is decaying in the early twenties, then that’s when our exercise intervention should actually start and it should continue until as late in life as possible. For those who are aged and sedentary, the sooner exercise is added into the lifestyle, the better. But which leg exercise should be recommended?
Leg extensions and leg curls are not the answer as they are isolation exercises and do not mimic normal daily activities nor do they tax the breadth of functional capability of the entire leg. Squats are the answer. Front, back, high bar, low bar, or any other complete range of motion free weight squat exercises done progressively two to three times per week is most preferable.
But not every aging person, or fitness or medical professional, thinks that the elderly can or should do a squat. The easiest, and oldest argument against this position is that if the individual can independently, in their current physical state, sit down on a toilet and get back up again, then they are fully capable of beginning a program of squat exercises; beginning from an easy challenge meeting the individual where they are at in terms of strength and ability, then slowly progressing in intensity and volume as tolerated by the elderly trainee.
But what about those who are not strong enough to sit on a toilet and stand up without the use of assistance rails? Well, this is the group – mostly the over 50s – where exercise machines such as the leg extension and leg curl become valuable. Both of these exercises are performed while seated which removes bodyweight from consideration. As such extremely low loads can be used. But use of these isolation exercises should be couched in progression, where load is slowly and progressively added until strength is such that the trainee can begin using the leg press machine. Again this is an exercise that removes bodyweight from the equation. Once the trainee can perform leg presses with about 133% of bodyweight for 5 to 10 repetitions, then a transition to learning and regularly doing squats should follow. A different approach can be used in that air squats (or bodyweight squats or deep knee bends) can be scaled down in range of motion and load to accommodate a trainee’s low work capacity to start, then they can be progressed slowly and as they successfully adapt in strength and mobility.
While the value of squatting becomes manifest fairly quickly, with obvious functional improvements in weeks, there will be some initial trainee trepidation; pain and low function are doubt inducing. To keep the trainee on the right road, we must convince the trainee that including the squat, even with extremely low starting loads, firmly places them on the path to restoring strength, mobility, and even endurance to the point that anatomical, physiological, physical, and social limitations to engagement in a normal life evaporate.
References used for graph construction:
- Amaral et al, Brazilian Journal of Physical Therapy 18(2): 183-190, 2014
- Forrest et al, The Aging Male 8(3): 151-156, 2005
- Gallagher et al, Journal of Shoulder and Elbow Surgery 6(4): 340-346, 1997
- Gulecyuz et al, Biomedical Research International 2117: 1654796, 2017
- Harbo et al, European Journal of Applied Physiology 112(1): 267-275, 2011
- Hughes et al, American Journal of Sports Medicine 27(5): 651-657, 1999
- Kallman et al, Journal of Gerontology 45(3): M82-88. 1990
- Keinbacher et al, Journal of Neuroengineering and Rehabilitation 13: 16, 2016
- Keinbacher et al, Journal of Rehabilitation and Medicine 48: 60-69, 2016
- Lauretani et al, Journal of Applied Physiology 95(5): 1851-1860, 1985
- Petrella et al, Journal of Applied Physiology 98(1): 211-220, 2005
- Pike et al, Journal of Joint and Elbow Surgery International 6(6): 1029-1033, 2022
- Pradhan et al, Journal of Physiological Anthropology 30: 11, 2020
- Sasaki et al, PLoS One 13(2): e0192687, 2018
Lon Kilgore earned a Ph.D. from the Department of Anatomy and Physiology at Kansas State University’s College of Veterinary Medicine. He has competed in weightlifting to the national and international level since 1972 and coached his first athletes from a garage gym to national-championship event medals in 1974. He has also competed in powerlifting and currently holds several continental and world records, won his division in the first CrossFit Total event, was a decent high school wrestler, caught a number of crabs during his short collegiate rowing stint, was and still is a hack at golf, and was a regional fish cutting champion and competitor at nationals. He has worked in the trenches – as a qualified national-level coach or scientific consultant – with athletes from rank novices to the Olympic elite, and as a consultant to fitness businesses. He was co-developer of the Basic Barbell Training and Exercise Science specialty seminars for CrossFit (mid-2000s) and was an all-level certifying instructor for USA Weightlifting for more than a decade. He is a decorated military veteran (sergeant, U.S. Army). His anatomical illustration, authorship, and co-authorship efforts include several bestselling books and works in numerous research journals. His fitness standards for weightlifting and calisthenics have been included in textbooks and multitudinous websites. After leaving a 20-year plus professorial career in higher academia, his teachings can be found in vocational-education courses offered through the Kilgore Academy, and in articles like these.

Support the Broken Science Initiative.
Subscribe today →
One Comment
recent posts

Flawed scientific thinking lies at the heart of postmodern scientific, medical, and institutional failures

Dr. Drew traces the roots of modern misinformation to scientific illiteracy and a growing intolerance for uncertainty, debate, and dissent.

How Broken Science Built the Chronic Disease Epidemic—and Why Education Is the Way Out



Good article. The awareness of strength loss as we age is an essential part of remaining healthy, but only if we take action to prevent or minimize this dynamic. While the article discusses ways to mitigate strength loss, “Dialing in . . . “, I would add and highly recommend a HIT program based on super slow by Ken Hutchins (Drew Baye) and the “Body By Science” book and program by Doug McGuff and John Little. Yes, these programs use machines and favor compound exercises to muscle failure that can be safely performed by anyone at any age. They also have free-weight equivalents for those who don’t have access to machines. It’s all good when the objective of health maintenance through muscle preservation becomes a key component of one’s lifestyle.